Total parenteral nutrition (TPN) is a feeding method that omits the gastrointestinal tract. Most of the body’s nutritional requirements are met by a specific formula that is administered intravenously. This technique is utilized when a person cannot receive feedings or fluids orally. A patient may require TPN permanently or temporarily, depending on the illness.
IV Fluids Fully in Stock
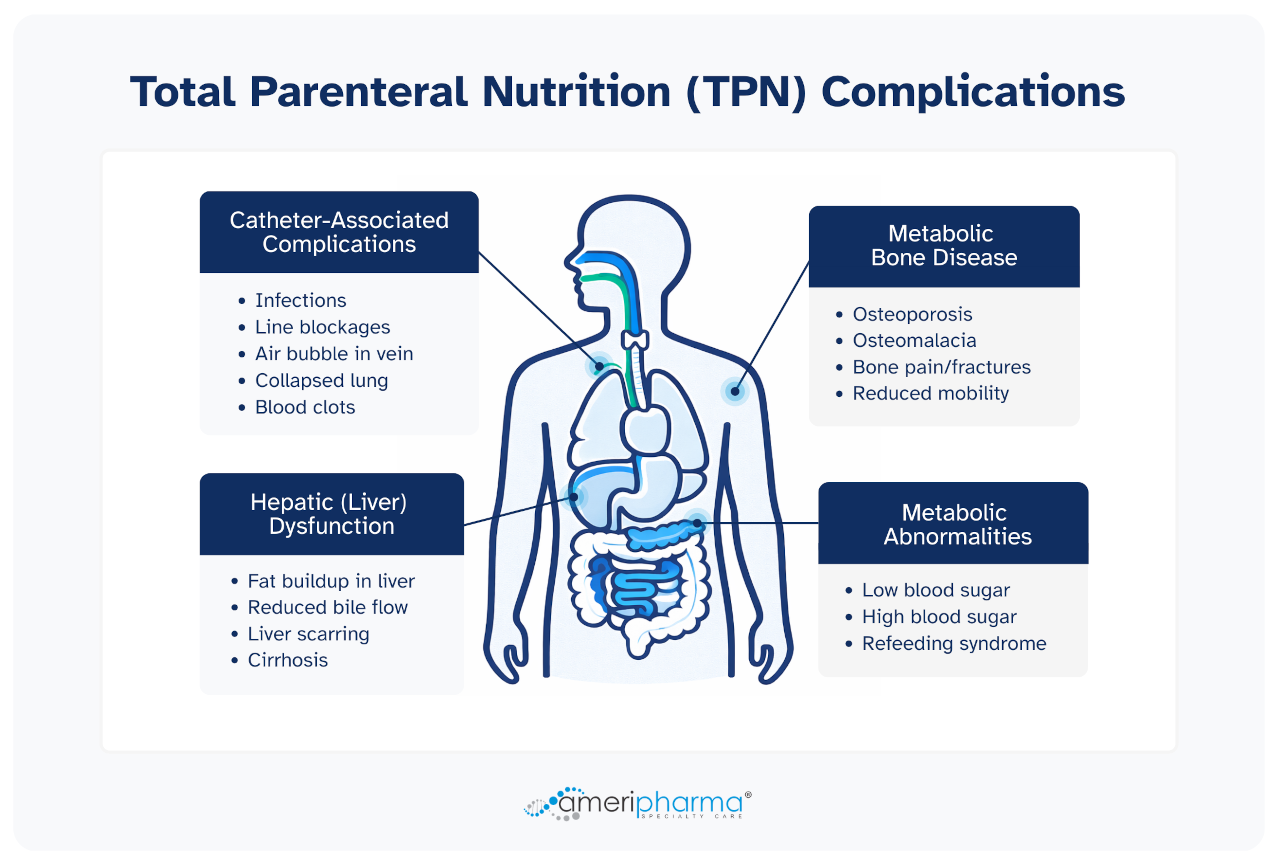
Reliable supply for uninterrupted carePoor aseptic techniques and poor maintenance of TPN central lines can lead to severe TPN complications [1]. It has been reported that about 5% to 10% of patients receiving total parenteral nutrition (TPN) have experienced adverse side effects and long-term complications associated with central venous access (central lines) or TPN itself [2]. Healthcare professionals have reported the following TPN complications:
- Catheter-associated complications
- Metabolic abnormalities
- Hepatic complications
- Metabolic bone disease
- Thrombosis (blood clots)
- Dehydration and electrolyte imbalances
- Infection
Catheter-associated TPN Complications
Catheter insertions are necessary for TPN feedings and may lead to catheter-related problems. Two complications that most frequently arise are infections and catheter occlusions. However, these complications can be avoided by keeping the lines clean and using the catheter only for TPN.
Other complications may include poor aseptic technique, contamination around the insertion area, and poor maintenance of central lines. Complications with central venous access affect 5% to 10% of individuals receiving TPN. The most frequent and potentially lethal catheter-associated complications experienced by patients during TPN nutritional support include acute bacterial infections called sepsis (bloodstream infection) and localized skin infections at the insertion or exit point of the catheter [1, 2].
Research statistics show that approximately 100,000 patients experienced 80–189 episodes of central line-associated bloodstream infection (CLABSIs) per year in the US due to poor aseptic techniques. The mortality rate of CLABSIs ranges between 12% to 25% of cases [3].
Amateur insertion of catheters in the veins can result in air embolisms (which happens when an IV tube is left unclamped or removed without being clamped, leading to the formation of air bubbles in the vein), pneumothorax (a condition in which your lungs collapse when the tip of a catheter enters into the pleural cavity), and thrombosis (blockage of a vein due to blood clots or injury) [2]. According to TPN guidelines, practicing aseptic techniques of insertion or removal of the catheter can help avoid catheter-associated complications. [4]
AmeriPharma® Specialty Care
Total Parenteral Nutrition | Leader In TPN AssistanceMetabolic Abnormalities

Approximately 90% of patients receiving TPN administration experience metabolic complications, specifically glucose abnormalities (hypoglycemia or hyperglycemia). Metabolic complications can be controlled by monitoring electrolytes, blood glucose levels, and insulin levels.
Metabolic complications (abnormalities) may arise due to rapid infusion of nutrients after a recent malnourished state. Some of the major metabolic abnormalities include hypoglycemia (which happens due to TPN discontinuation) or hyperglycemia and refeeding syndrome (severely malnourished patients experience this syndrome usually within 24 to 48 hours when TPN infusion results in metabolic and hormonal changes characterized by electrolytes shift.) [5, 6] When starting TPN in previously malnourished patients, refeeding syndrome is caused by abrupt changes in fluid and electrolyte levels. Refeeding syndrome patients typically have low levels of phosphate, magnesium, and potassium. These symptoms may become exacerbated with TPN, largely caused by low levels of phosphate, leading to respiratory failure, convulsions, delirium, and death. It can also decrease cardiac contractility.
Hepatic Complications
Total parenteral nutrition can result in a plethora of hepatic complications. Some of the hepatic complications include hepatic steatosis, gallbladder and bile duct damage, and cholestasis. The most serious consequence can lead to progressive fibrosis and cirrhosis, which is the most notable concern in long-term use of TPN in both adults and pediatric patients. Long-term TPN use can lead to low birth weight, sepsis, short bowel syndrome, and prematurity.
Hepatic complications are more prevalent in infants with immature liver but can occur at any age, affecting 15% to 40% of patients receiving total parenteral nutrition (TPN) infusion. Hepatic complications include liver dysfunction, increased ammonia levels, and painful hepatomegaly.
- Liver dysfunction commonly occurs due to an increased ratio of bilirubin and alkaline phosphatase, resulting in inflammation, cholestasis, and progressive fibrosis.
- Increased ammonia levels and painful hepatomegaly result in fat accumulation, feeling of twitching, seizures, and lethargy.
If you experience one of those symptoms, consult your doctor immediately. Healthcare professionals usually reduce protein delivery during these complications [5].
Speak to a Specialist About Copay Assistance
Metabolic Bone Disease
Metabolic bone disease is a problem that can arise in long-term TPN use. Approximately 40% of the patient’s receiving long-term TPN infusion experience metabolic bone diseases such as osteomalacia and osteoporosis. This can lead to a decrease in quality of life due to bone pain, fractures, and limited mobility. However, the prevalence and pathogenesis of bone demineralization are still unclear [5]. The reported causes of these bone diseases can be due to:
- Less exposure to sunlight (low vitamin D intake)
- Lack of physical activity
- Side effects of other therapies such as heparin and steroids
- Suboptimal intake of calcium, phosphate, and vitamin D
It has been demonstrated that intravenous pamidronate improves the bone mineral density of patients receiving TPN at home [7].
REFERENCES:
- Maudar KK. Total parenteral Nutrition. Elsevier. 1995; 51 (2):122-126
- Kornbau C, Lee KC, Hughes GD, Firstenberg MS. Central line complications. International Journal of Critical Illness and Injury Science. 2015 Jul;5 (3):170.
- To KB, Napolitano LM. Common complications in the critically ill patient. Surgical Clinics. 2012 Dec 1;92(6):1519-57.
- Doyle GR, McCutcheon JA. Clinical Procedures for Safer Patient Care Clinical Procedures for Safer Patient Care: Chapter 8. Campus Manitoba. 2016; 1.
- Hartl WH, Jauch KW, Parhofer K, Rittler P, Working Group for Developing the Guidelines for Parenteral Nutrition of the German Association for Nutritional Medicine. Complications and monitoring–guidelines on parenteral nutrition, Chapter 11. GMS German Medical Science. 2009;7.
- Sobotka L, Camilo ME. Basics in clinical nutrition: Metabolic complications of parenteral nutrition. e-SPEN, the European e-Journal of Clinical Nutrition and Metabolism. 2009; 3(4):e120-2.
- Nishikawa RA, Siepler SE, Siepler JK, Diamantidis T, Okamoto R. Intravenous pamidronate improves bone mineral density in home parenteral nutrition patients. Clinical Nutrition. 2003(22):S88.