




Overview of Intravenous Immunoglobulin (IVIG) vs. Subcutaneous Immunoglobulin (SCIG)
Immunoglobulin (IG) replacement therapy has become the cornerstone of primary immunodeficiency (PI) disease treatment in patients who have defects in their body’s antibody production. Antibodies play a vital role in our immune system. They act as our defense system against foreign substances that are introduced to our bodies, such as viruses, bacteria, and other substances.
Get IVIG Prior Authorization
SCIG and IVIG are prepared from the blood donated by thousands of human donors, yielding a concentrated and diverse mixture of antibodies that can protect recipients against many possible infectious organisms.
IG can be either administered through an intravenous (IV) line or administered subcutaneously (SC) under the skin. While IVIG causes a rapid rise in serum IG, SCIG does not. IVIG also has more side effects than SCIG.
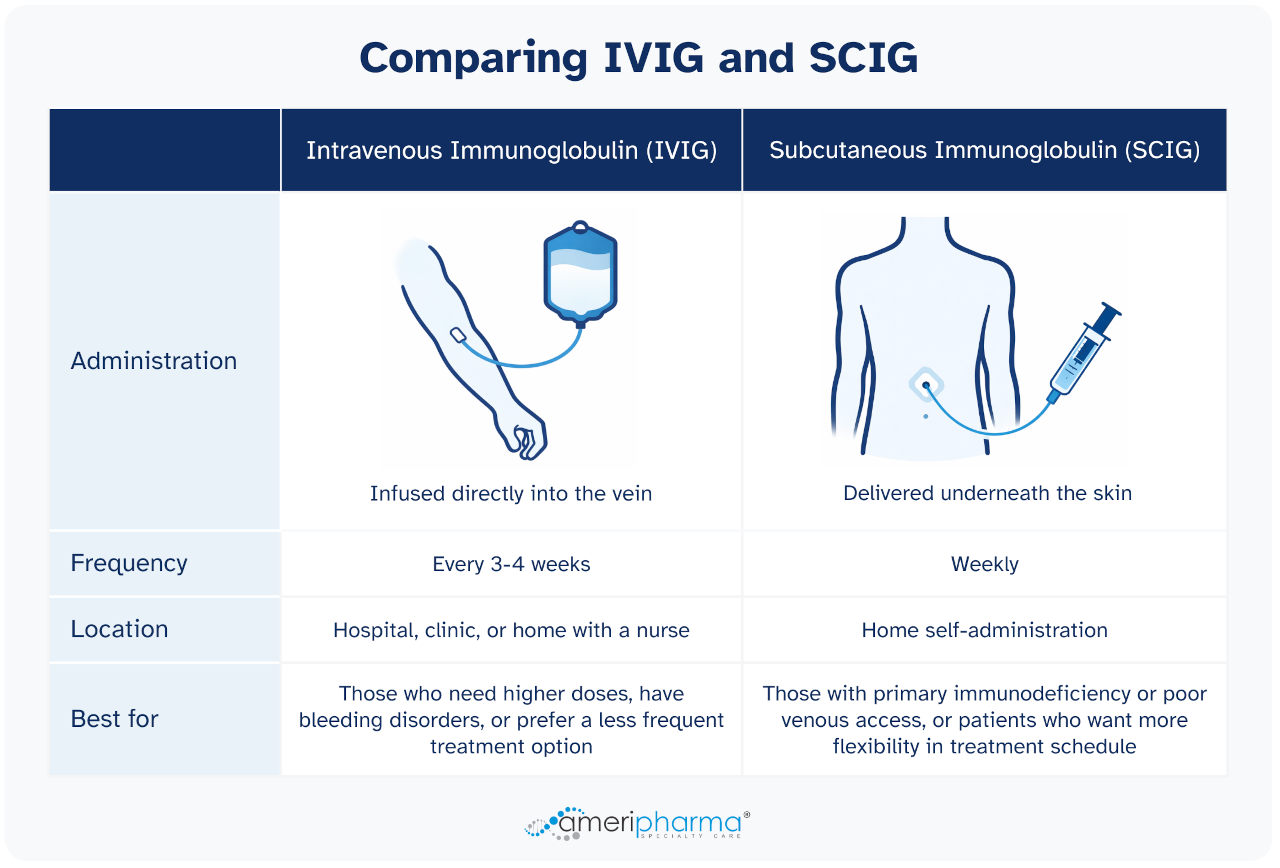
IVIG is given into a vein (intravenously) as an infusion that can usually take from 1 to 4 hours or even longer, depending on the dose and other factors involving the patient’s health. Upon IVIG infusion, the serum IG levels increase rapidly, achieving peak serum concentrations in about 15 minutes after the infusion, followed by a sharp drop in serum levels over the following 48 hours.
SCIG is given by slowly injecting immunoglobulin into the fatty tissue that is just underneath the skin. IG administered subcutaneously eventually makes its way into the circulation at a much slower rate with IVIG, resulting in more stable serum IG levels, avoiding the “peak” IG levels that usually accompany IVIG infusions.
There is no evidence that either method of administration is more effective than the other. So why would you choose one over the other? In order to answer this question, it is necessary to look at the advantages that IVIG and SCIG offer in comparison to one another.
Advantages of IVIG vs. SCIG
- IVIG usually only needs to be infused once every 3 to 4 weeks, as opposed to the weekly infusions of SCIG.
- It can achieve rapid plasma levels (medication exhibits its effect faster).
- It can be used in patients with bleeding disorders.
- It is more suitable for higher doses as it allows for larger volumes to be infused (e.g., 2 gm/kg doses).
- It doesn’t need any experience on the patient’s end as it either gets infused at the doctor’s office, infusion center, or, if approved, at the patient’s home in the presence of an infusion nurse who handles the administration of the medication.
- It generally involves less needle pricking as it needs only one IV access, and this process is only repeated once every 3 to 4 weeks.
- It generally has fewer local reactions, such as pain, redness, and swelling, than with SCIG.
- It is more suitable for patients who have more difficulty handling needles or for some parents who feel less comfortable infusing their young children frequently.
Get IVIG Copay Assistance
Speak to a SpecialistAdvantages of SCIG vs. IVIG
- It has fewer systemic adverse effects (better tolerability than IVIG).
- It provides more even IG levels compared to IVIG (lack of peak and trough effect as in IVIG).
- It doesn’t require hospital-based infusion settings (The patient can self-infuse at home without the need for venous access.)
- It offers more flexibility in terms of the patient’s schedule.
- It is usually appropriate for patients with PI as they generally require lower doses of IG.
- It is more suitable for patients with poor venous access (hard stick patients).

SCIG generally exhibits fewer systemic adverse reactions, such as headache, nausea, vomiting, fever, and chills, which can be very disturbing even though they are not life-threatening. Studies have shown that the rate of non-serious systemic adverse reactions in patients on SCIG is about one-third to one-half the rate with IVIG. Pretreatment before IVIG infusion with antihistamines, acetaminophen, and in some cases, systemic steroids are widely used but are rarely needed with SCIG infusions.
SCIG is also generally well-tolerated by most patients who previously had serious systemic reactions to IVIG, and this is most likely related to the slower rate at which the SCIG is absorbed into circulation, which prevents high peaks in serum IG that occur with IVIG infusions.
SCIG given at weekly infusions provides more even serum IG levels and avoids the low trough levels that usually occur near the end of the 3- or 4-week infusion schedule of IVIG, a period in which some patients can become more susceptible to infections. For the same reason, patients who are on weekly SCIG are less likely to have fatigue, muscle, and joint pains in those same trough periods (“wear-off” periods).
SCIG provides patients with a sense of autonomy and allows them to be free from repetitive trips to hospitals, infusion centers, or other medical facilities, and in such a way, reduces their exposure to nosocomial infections. Infusions can be scheduled after school or work or during the evenings. Studies have shown that SCIG therapy has resulted in fewer missed work and school days than IVIG therapy in PI patients.
SCIG does not require IV access, which can be a challenge for IVIG patients who have difficulty getting their veins accessed, and even though they can get IV ports or PICC lines inserted to facilitate their infusions, this puts them at greater risk for infection.
Get Your IVIG Dose
At-Home InfusionIVIG vs. SCIG: Making the Right Choice for the Patient
IV and SC routes have both been proven to have similar efficacy when treating patients with primary immunodeficiency. The route of administration of immunoglobulin therapy should be based on patient attributes as well as their medical conditions. It is always a good idea to discuss different routes of administration with your doctor and ask if more than one option is suitable for you.
Available IG products are usually route-specific. Some are only approved for IV administration, and others only for subcutaneous administration. There are some products that have been approved for both IV as well as SC administration.
Patients treated with SCIG have the convenience of home-based IG administration, in which they get to choose the time and place of administration. In comparison, IVIG administration at a healthcare institution allows for frequent contact with healthcare professionals during the administration process, leading to better clinical monitoring and administration outcomes. It is important that you visit your doctor at an appropriate frequency so they may be able to continuously monitor your labs and follow your therapy and modify your therapy if there is ever a need for it.
It is good to know that even with IVIG, there are different options as to where you can get your infusions done, and this may offer you more flexibility. These options are:
- Hospital inpatient/outpatient (IVIG)
- Physician’s office (IVIG)
- Outpatient infusion center (IVIG)
- Home-based infusion (IVIG/SCIG)
Each of the above-mentioned administration locations will require either a doctor or nurse on site.
Whether a patient gets their immunoglobulin infusion done intravenously or subcutaneously, both therapies can be very efficacious, and the treatment success will be dependent on the collaborative effort between the patient and their clinician. Both IV and SC routes of administration are indicated and clinically appropriate for use in patients with primary immunodeficiency (PI). Patients should discuss both treatment options with their physicians and understand the risk and benefits of the different options. This would be very helpful in deciding on a regimen that would be most fitting and well-suited for the patient.
Can IVIG help?
Free IVIG Treatment InfoPublicly Available Reports on Patient Preferences
In several studies, patients who switched from IVIG to SCIG were asked which method they preferred.
In a 2006 US-Canada study, 81% of patients preferred SCIG vs. IVIG, while 19% preferred IVIG. A 2008 study found that 100% of Swedish patients preferred SCIG. In a recent study of 82 European patients, 92% preferred SCIG, and 8% preferred IVIG. Thus, it appears that most patients who try SCIG prefer it over IVIG.
Patients with autoimmune or neuropathic disorders other than PI (e.g., myasthenia gravis, MMN, CIDP, dermatomyositis) who receive high-dose therapy should know that SCIG seems to be effective for these conditions. However, there is still a lack of research on whether SCIG is as effective as IVIG.
REFERENCES:
- Walter G, Kalicinsky C, Warrington R, Miguel M, Reyes J, Rubin TS. Delivery of subcutaneous immunoglobulin by rapid “push” infusion for primary immunodeficiency patients in Manitoba: a retrospective review. Allergy Asthma Clin Immunol. 2020 May 13;16:34. doi: 10.1186/s13223-020-00431-3. PMID: 32426003; PMCID: PMC7218483.
- Kobayashi RH, Gupta S, Melamed I, Mandujano JF, Kobayashi AL, Ritchie B, Geng B, Atkinson TP, Rehman S, Turpel-Kantor E, Litzman J. Clinical Efficacy, Safety and Tolerability of a New Subcutaneous Immunoglobulin 16.5% (Octanorm [Cutaquig®]) in the Treatment of Patients With Primary Immunodeficiencies. Front Immunol. 2019 Feb 4;10:40. doi: 10.3389/fimmu.2019.00040. PMID: 30778345; PMCID: PMC6369354.
- Ochs HD, Gupta S, Kiessling P, Nicolay U, Berger M; Subcutaneous IgG Study Group. Safety and efficacy of self-administered subcutaneous immunoglobulin in patients with primary immunodeficiency diseases. J Clin Immunol. 2006 May;26(3):265-73. doi: 10.1007/s10875-006-9021-7. PMID: 16783465.
- Moore ML, Quinn JM. Subcutaneous immunoglobulin replacement therapy for primary antibody deficiency: advancements into the 21st century. Ann Allergy Asthma Immunol. 2008 Aug;101(2):114-21; quiz 122-3, 178. doi: 10.1016/S1081-1206(10)60197-4. PMID: 18727465
- Gardulf A, Nicolay U, Asensio O, Bernatowska E, Böck A, Carvalho BC, Granert C, Haag S, Hernández D, Kiessling P, Kus J, Pons J, Niehues T, Schmidt S, Schulze I, Borte M. Rapid subcutaneous IgG replacement therapy is effective and safe in children and adults with primary immunodeficiencies–a prospective, multi-national study. J Clin Immunol. 2006 Mar;26(2):177-85. doi: 10.1007/s10875-006-9002-x. Epub 2006 Apr 26. PMID: 16758340.
- Gardulf A, Nicolay U, Math D, Asensio O, Bernatowska E, Böck A, Costa-Carvalho BT, Granert C, Haag S, Hernández D, Kiessling P, Kus J, Matamoros N, Niehues T, Schmidt S, Schulze I, Borte M. Children and adults with primary antibody deficiencies gain quality of life by subcutaneous IgG self-infusions at home. J Allergy Clin Immunol. 2004 Oct;114(4):936-42. doi: 10.1016/j.jaci.2004.06.053. PMID: 15480339.
- Nicolay U, Kiessling P, Berger M, Gupta S, Yel L, Roifman CM, Gardulf A, Eichmann F, Haag S, Massion C, Ochs HD. Health-related quality of life and treatment satisfaction in North American patients with primary immunodeficiency diseases receiving subcutaneous IgG self-infusions at home. J Clin Immunol. 2006 Jan;26(1):65-72. doi: 10.1007/s10875-006-8905-x. PMID: 16418804.
- Fasth A, Nyström J. Quality of life and health-care resource utilization among children with primary immunodeficiency receiving home treatment with subcutaneous human immunoglobulin. J Clin Immunol. 2008 Jul;28(4):370-8. doi: 10.1007/s10875-008-9180-9. Epub 2008 Feb 7. PMID: 18256911.
- Hoffmann F, Grimbacher B, Thiel J, Peter HH, Belohradsky BH; Vivaglobin Study Group. Home-based subcutaneous immunoglobulin G replacement therapy under real-life conditions in children and adults with antibody deficiency. Eur J Med Res. 2010 Jun 28;15(6):238-45. doi: 10.1186/2047-783x-15-6-238. PMID: 20696632; PMCID: PMC3351992.
- https://www.genome.gov/genetics-glossary/Antibody
- https://igcares.com/home/education-scig-vs-ivig.html
- https://www.ajmc.com/view/intravenous-and-subcutaneous-immunoglobulin-treatment-options












